Urticaria and Angioedema
A detailed discussion is beyond the
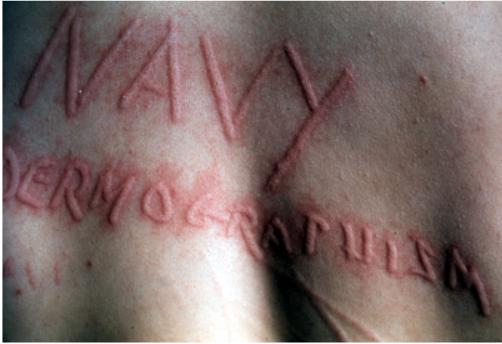
scope of this chapter. Urticaria (hives) can be conceptualized as
being massive acute migratory dermal edema, usually extremely itchy.
Angioedema on the other hand involves the deeper dermis and the
subcutaneous fat frequently in the eyelids, lips, hands, and feet. Acute urticaria and angioedema is seen
in patients with anaphylaxis, serum sickness or as a reaction to
arthropod bites, medications, infections, vaccinations, and foods.
Urticaria that persists beyond 6 weeks has been defined as chronic
urticaria. This discussion is limited to typical acute urticaria or
angioedema, which does not involve vascular instability, dyspnea, or
other systemic manifestations. (a) Etiologies to consider in the
active duty age group Medications - beta lactams (especially
penicillins), sulfa, NSAIDs, opiates, radio contrast dye, douches, and
OTC cold preparations (to name only a few). Infections - for acute urticaria in
the active duty age group consider: incubating hepatitis,
mononucleosis, influenza, viral gastroenteritis, viral URI, atypical
pneumonia, UTI, strep throat, dental manipulation, vaginitis, otitis,
inflammatory tinea, scabies, and intestinal parasites.
Foods - peanuts, strawberries,
seafood, nuts, berries, bananas, grapes, tomatoes, cheese, eggs, and
food coloring (to name a few). (b) Treatment Epinephrine - use 0.3-0.5 mg IM (if
skin involvement is very severe or if lips, eyelids, larynx,
bronchospasm and/or hypotension occurs) Antihistamines - diphenhydramine 50 mg
IM or orally; the effects are not immediate. Follow up with regular
oral use of hydroxyzine 10-50 mg or diphenhydramine 25 -100 mg QID.
Remember these drugs are sedating. Alternatively, the non-sedating
antihistamine loratidine (Claritin) 10 mg QD, certrizine (Zyrtec) 5 or
10 mg QD or fexofenidine (Allegra) 60 mg BID may be used for
maintenance.
Be alert that some non-sedating drugs
can still sedate certain patients. If special military duty is
involved, be sure to check with a flight surgeon or undersea medical
officer. Topical Corticosteroids - not
effective. Systemic steroids – these have a very
delayed onset of action and are not first line drugs for a typical case of
acute urticaria or angioedema. Consider prescribing this medication only if
antihistamines taken during the entire day do not suppress the eruption. In most cases a couple of weeks of round the
clock therapy are all that is needed. If the urticaria is recurrent, severe
or uncontrollable, then the patient should be referred to a dermatologist or
allergist for evaluation. Do not be surprised if the evaluation by the
specialist is negative. It is almost the uniform experience of dermatologists
that a "smoking gun" is the exception rather than the rule. This is difficult
for patients (and concerned supervisors and commanders) to understand and
accept. Nonetheless, it is a fact. Written and revised by CAPT Dennis A. Vidmar, MC, USN, Department of Military and Emergency Medicine, and Department of Dermatology, Uniformed Services University of the Health Sciences, Bethesda, MD (1999). Additional images provided by CAPT Vidmar in June, 2000, subsequent to the initial publication of this manual. |


Preface · Administrative Section · Clinical Section
The
General Medical Officer Manual , NAVMEDPUB 5134, January 1, 2000
Bureau
of Medicine and Surgery, Department of the Navy, 2300 E Street NW, Washington, D.C.,
20372-5300
This web version of The General Medical Officer Manual, NAVMEDPUB 5134 is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy version, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. All material in this version is unclassified. This formatting © 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved.
Home · Textbooks and Manuals · Videos · Lectures · Distance Learning · Training · Operational Safety · Search
|
|
|
This website is dedicated to the development and dissemination of medical information that may be useful to those who practice Operational Medicine. This website is privately-held and not connected to any governmental agency. The views expressed here are those of the authors, and unless otherwise noted, do not necessarily reflect the views of
the Brookside Associates, Ltd., any governmental or private organizations. All writings, discussions, and publications on this website are unclassified.
© 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved
Other Brookside Products
![]()