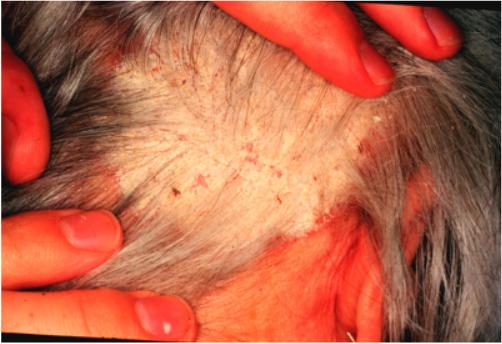
Psoriasis and Seborrheic Dermatitis
Like atopic dermatitis and endogenous hand eczema, psoriasis and its variants are listed as disqualifying for entry and the pursuit of certain special duty in the Armed Forces of the United States. The reasons are the same as eczema; the notorious unpredictability of the condition. A case of clinically banal psoriasis can sometimes explode into disease of a debilitating nature in the military environment. Waivers should be very judiciously granted for this condition only after consultation with a military dermatologist. The "three legged stool" of medication, lubrication, and environmental control applies equally well to the treatment of psoriasis (see Eczema above). The novice primary care practitioner inappropriately neglects lubrication in favor of potent topical steroids. Psoriasis perpetuates itself on dry cracked skin. Moisturize, moisturize, and moisturize! Topical steroids are not a substitute for emollients. Scalp lesions are best approached with sulfur/salicylic acid, zinc pyrithione, or coal tar based medicated shampoos. The key to success here is sufficient contact time. The shampoo must have several minutes in place on the scalp before rinsing. There are a large number of generic and proprietary products on the market: Tarsum, T-Gel, Pentrax, Sebulex, Sebutone, and other dandriff shampoo brands to name but a few. Ketoconazole shampoo is also useful, but is best saved for situations where conventional shampoos do not help. This product is very expensive and should be used judiciously. Topical steroid lotions (e.g. betamethasone valearate 0.1%) applied after shampoo are a nice way to deliver medication to lesions within and near hair bearing surfaces such as the scalp and eyebrows. Do not use systemic steroids to control psoriasis. An impressive "rebound" usually occurs which can be very difficult to treat. Scalp lesions (i.e., dandruff) are treated the same as psoriasis (see Psoriasis above). The areas of greasy scale with background erythema on the central face, forehead, retroauricular, genitalia, and periumbilical locations should be treated with a low potency steroid cream or ointment (e.g., hydrocortisone 1% or desonide 0.05%). Written and revised by CAPT Dennis A. Vidmar, MC, USN, Department of Military and Emergency Medicine, and Department of Dermatology, Uniformed Services University of the Health Sciences, Bethesda, MD (1999). Additional images provided by CAPT Vidmar in June, 2000, subsequent to the initial publication of this manual. |
|



Preface · Administrative Section · Clinical Section
The General Medical Officer Manual , NAVMEDPUB 5134, January 1, 2000
Bureau of Medicine and Surgery, Department of the Navy, 2300 E Street NW, Washington, D.C., 20372-5300
This web version of The General Medical Officer Manual, NAVMEDPUB 5134 is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy version, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. All material in this version is unclassified. This formatting © 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved.
Home · Textbooks and Manuals · Videos · Lectures · Distance Learning · Training · Operational Safety · Search
|
|
|
This website is dedicated to the development and dissemination of medical information that may be useful to those who practice Operational Medicine. This website is privately-held and not connected to any governmental agency. The views expressed here are those of the authors, and unless otherwise noted, do not necessarily reflect the views of the Brookside Associates, Ltd., any governmental or private organizations. All writings, discussions, and publications on this website are unclassified.
© 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved
Other Brookside Products
![]()