|
|
|
Operational Obstetrics & Gynecology
Labor and Delivery
Watch a Video Showing a Normal Delivery or Cesarean Section
For a woman experiencing her first baby, labor usually lasts about 12-14 hours. If she has delivered a baby in the past, labor is generally quicker, lasting about 6-8 hours. These averages are only approximate, and there is considerable variation from one woman to the next, and from one labor to the next.
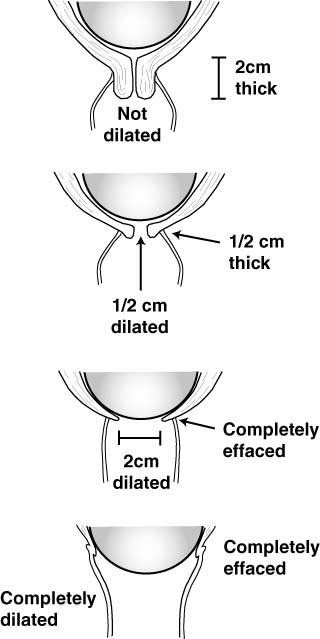
During labor, the cervix dilates (opens) and effaces (thins). This process has been likened to the process of pulling a turtleneck sweater over your head. The collar opens (dilates) to allow your head to pass through, and also thins (effaces) as your head passes through.
The process of dilatation and effacement occurs for both mechanical reasons and biochemical reasons.
 The force of the contracting uterus naturally seeks to dilate and thin the cervix.
However, for the cervix to be able to respond to these forces requires it to be
"ready." The process of readying the cervix on a cellular level usually takes
place over days to weeks preceding the onset of labor.
The force of the contracting uterus naturally seeks to dilate and thin the cervix.
However, for the cervix to be able to respond to these forces requires it to be
"ready." The process of readying the cervix on a cellular level usually takes
place over days to weeks preceding the onset of labor.
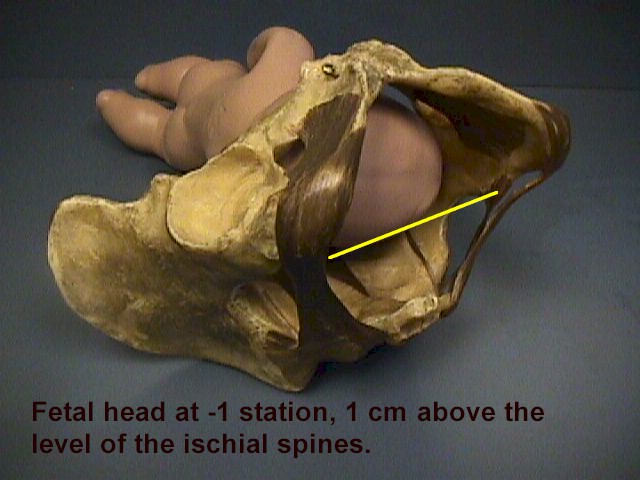
Descent means that the fetal head descends through the birth canal. The "station" of the fetal head describes how far it has descended through the birth canal.
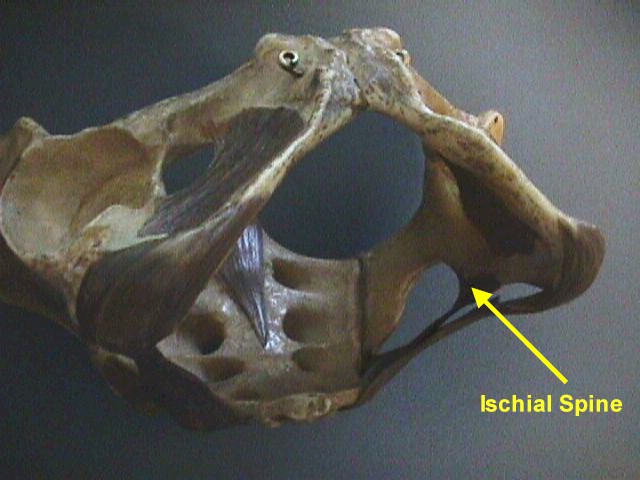
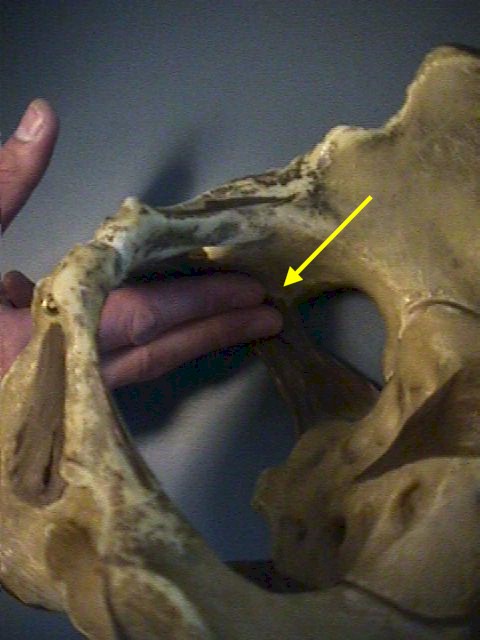
This station is determined relative to the maternal ischial spines, bony prominences on each side of the maternal pelvic sidewalls.
"0 Station" ("Zero Station") means that the top of the fetal head has descended through the birth canal just to the level of the maternal ischial spines.
This usually means that the fetal head is "fully" engaged (or "completely engaged"), because the widest portion of the fetal head has entered the opening of the birth canal (the pelvic inlet).
 |
 |
 |
If the fetal head has not reached the ischial spines, this is indicated by negative numbers, such as -2 (meaning the top of the fetal head is still 2 cm above the ischial spines).
If the fetal head has descended further than the ischial spines, this is indicated by positive numbers, such as +2 (meaning the top of the head is now 2 cm below the ischial spines).
Negative numbers above -3 indicate the fetal head is unengaged (floating). Positive numbers beyond +3 (such as +4 or +5) indicate that the fetal head is crowning and about to deliver.
Women having their first baby often demonstrate deep engagement (0 or +1) for days to weeks prior to the onset of labor.
Women having their second or third baby may not engage below -2 or -3 until they are in labor, and nearly completely dilated.
Home · Introduction · Medical Support of Women in Field Environments · The Prisoner of War Experience · Routine Care · Pap Smears · Human Papilloma Virus · Contraception · Birth Control Pills · Vulvar Disease · Vaginal Discharge · Abnormal Bleeding · Menstrual Problems · Abdominal Pain · Urination Problems · Menopause · Breast Problems · Sexual Assault · Normal Pregnancy · Abnormal Pregnancy · Normal Labor and Delivery · Problems During Labor and Delivery · Care of the Newborn
|
Bureau of Medicine
and Surgery |
Operational
Obstetrics & Gynecology - 2nd Edition |
This web version of Operational Obstetrics & Gynecology is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy NAVMEDPUB 6300-2C, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. All material in this version is unclassified.
This formatting © 2006
Medical Education Division,
Brookside Associates, Ltd.
All rights reserved