FMST Student Manual - 2008 Web Edition*
UNITED STATES MARINE CORPS
Field Medical Training Battalion
Camp Lejeune
FMST 1418
Perform Emergency Cricothyroidotomy
Terminal Learning
Objectives
1. Given
a casualty that meets the needs for an emergency Cricothyroidotomy in a combat
environment and standard field medical equipment and supplies, perform an
emergency Cricothyroidotomy to prevent further injury or death. (FMST-HSS-1418)
Enabling Learning
Objectives
1.
Without the aid of references, given a description or list, identify important
anatomical landmarks for an Emergency Cricothyroidotomy, per the student
handout. (FMST-HSS-1418a)
2. Without
the aid of references, given a description or list, identify the indications for
performing an Emergency Cricothyroidotomy, per the student handout.
(FMST-HSS-1418b)
3. Without
the aid of references, given a description or list, identify the
contra-indications for performing an Emergency Cricothyroidotomy, per the
student handout. (FMST-HSS-1418c)
4. Without
the aid of references, given a description or list, identify the proper
equipment for performing an Emergency Cricothyroidotomy, per the student
handout. (FMST-HSS-1418d)
5. Without
the aid of references, given a description or list, identify the procedural
sequence for Emergency Cricothyroidotomy, per the student handout.
(FMST-HSS-1418e)
6. Without
the aid of references, given a description or list, identify potential
complications of Emergency Cricothyroidotomy, per the student handout.
(FMST-HSS-1418f)
7. Without
the aid of references, given a simulated casualty and standard field medical
equipment and supplies, perform an Emergency Cricothyroidotomy, per the student
handout. (FMST -HSS-1418g)
1. DEFINITION
Emergency cricothyroidotomy is a surgical procedure where an
incision is made through the skin and cricothyroid membrane. This allows
for the placement of an endotracheal tube into the trachea when control of
the airway is not possible by other methods.
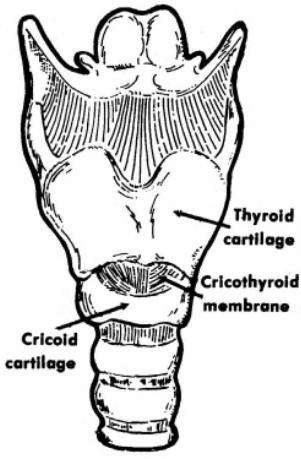
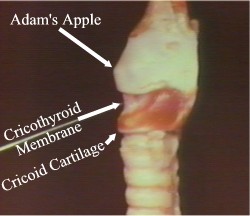
2. CRICOTHYROIDOTOMY
ANATOMICAL LANDMARKS (see figure 1)
Trachea - also known as the
windpipe. It is the cartilaginous and membranous tube descending from, and
continuous with, the lower part of the larynx to the bronchi.
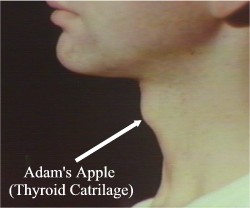
Thyroid Cartilage - also known as
the “Adam’s Apple.” The thyroid cartilage is located in the upper part of the
throat. The thyroid cartilage tends to be more prominent in men than women.
Cricoid Cartilage - located
approximately ¾-inch inferior to the thyroid cartilage. The cricoid and thyroid
cartilage form the framework of the larynx.
Cricothyroid Membrane - soft tissue
depression between the thyroid and cricoid cartilage. This membrane connects
the two cartilages and is only covered by skin.
Carotid Arteries - two principal
arteries of the neck
Jugular Veins - two principal veins
of the neck
Esophagus - musculo-membranous tube
extending downward from the pharynx to the stomach. The esophagus lies
posterior to the trachea.
Thyroid Gland - largest endocrine
gland, the thyroid gland is situated in front of the lower part of the neck.
Consists of a right and left lobe on either side of the trachea.
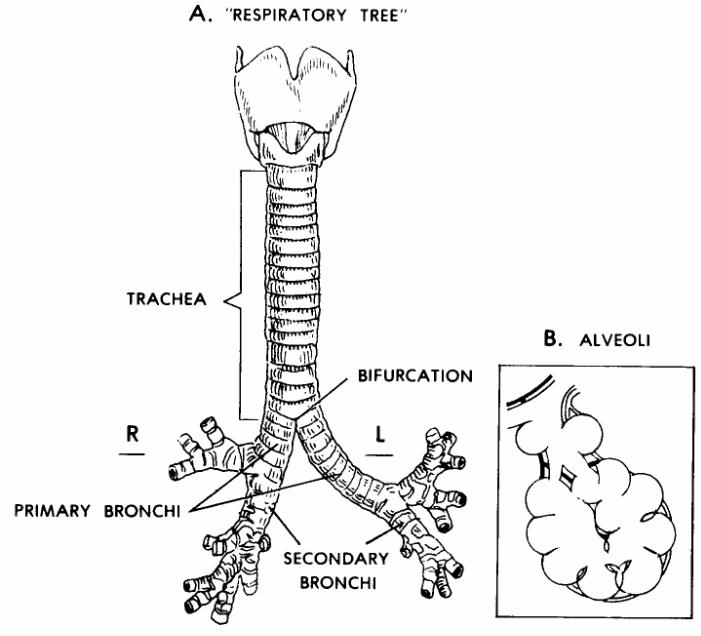
Substitute Figure 1. Anatomy of the Respiratory System*
|
3. INDICATIONS
There are many reasons an emergency cricothyroidotomy may be
required. Listed below are a few of the most common reasons:
Obstructed airway - obstructed
airway and/or swelling of tissues will usually prevent the passage of an
endotracheal tube through the airway. Therefore, a surgical airway distal to
the obstruction is required. Causes of an obstructed airway include:
a.
Facial and oropharyngeal edema from burns
b.
Foreign objects (food or teeth)
Congenital deformities of the
oropharynx or nasopharynx will inhibit or prevent nasotracheal or orotracheal
intubation.
Trauma to the head and neck would preclude the use of
an ambu-bag, oropharyngeal airway, nasopharyngeal airway, and endotracheal tube
insertion.
Examples include:
- Facial and oropharyngeal edema from severe trauma
- Facial fractures (mandible fracture)
- Nasal bone fractures
- Cribiform fractures
Cervical spine fractures in a
patient who needs an airway but whose intubation is unsuccessful or
contraindicated.
Last
resort - healthcare provider is unable to establish an
airway by any other means.
4.
ADVANTAGES/DISADVANTAGES
Advantages of Emergency Cricothyroidotomy
-
Provides a definitive airway for ventilating the patient.
- Can be performed quickly and has few complications associated
with the procedure.
Disadvantages
of Emergency Cricothyroidotomy
- Need
advanced training to properly perform procedure.
-
Bypasses the nares function of warming and filtering the air.
- May increase respiratory
resistance.
-
Improper placement.
- Casualty is now totally dependent on Corpsman
5.
PROCEDURAL STEPS
a.
Make your decision
- Look,
listen, and feel
-
Attempt to secure airway by all other means
- Justify your decision
b.
Assemble and Check Equipment (see figure 2)
- #11
scalpel blade
-
Scalpel blade handle
-
Endotracheal tube - shortened
- 10 cc
syringe - used to fill the cuff at the end of the endotracheal tube
- Stylet - a wire inserted into the endotracheal tube in order to
stiffen the tube during passage
- Water
soluble lubrication - KY Jelly or Surgilube
-
Stethoscope - to check for proper placement of the
endotracheal tube
-
Curved Kelly hemostat - used to open the incision site
- Tissue Forceps - used to retract skin tissue
at the incision site
- Ambu-bag - to ventilate patient
- Sterile dressing
- Petroleum gauze
- Betadine or alcohol wipes
- Sterile or clean gloves
- Suture material
- Suction device
- Suture scissors
- Tape
- Sterile dressing
|

Substitute Figure 2. Required Equipment* |
c.
Prepare patient
- Place
patient in a supine or semi-recumbent position.
- The
neck is placed in a neutral position.
-
Explain procedure (if the patient is conscious).
|

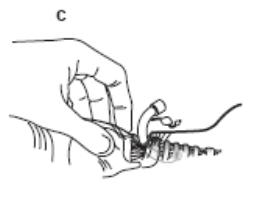
Use your index finger to identify the cricothyroid membrane, the soft
indentation just below the Adam's apple.

Stabilizing the trachea with thumb and forefinger, make a transverse
incision through the skin, over the membrane.

Push the scalpel straight down through the cricothyroid membrane. You will
feel a "pop" as you pass into the trachea.

Place a tube or tube-like device into the trachea to keep the airway open.

You may need to improvise.

Tape the airway in place.
From: Operational
Medicine, Health Care in Military Settings, NAVMED P-5139, January 1, 2001 |
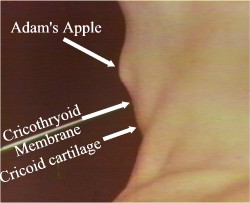
d.
Locate membrane
-
Palpate thyroid and cricoid cartilage for orientation (see figure 3).
-
Locate cricothyroid membrane.
-
Cleanse the incision site with alcohol or betadine swabs.
|

Substitute Figure 3.* |
e.
Make Incision
-
Stabilize the thyroid cartilage using your non-dominant hand.
- Make
a vertical incision through the skin approximately 2.5 cm (1 inch) long over the
cricothyroid membrane
-
Visualize the cricothyroid membrane.
- Enter
cricothyroid membrane.
- Make
a horizontal incision through the cricothyroid membrane (see figure 4).
- DO NOT make the incision more than ½ inch deep or you may
perforate the esophagus.
|

Substitute Figure 4. Horizontal Incision over the
Cricothyroid Membrane* |
f.
Open Incision
- Using either Kelly hemostat or knife blade handle, insert into
incision and blunt dissect incision (turn the curved Kelly hemostat 90 degrees
to open up the incision)
g. Insert Tube
- Insert the shortened endotracheal tube into the incision,
directing the tube distally down the trachea (see figure 5).
|
Substitute Figure 5.* |
Inflate
balloon with 10 cc’s of
air, this serves two purposes:
- Holds
the endotracheal tube in place.
- Acts as a barrier and prevents fluids from entering the lungs.
Ventilate the patient with two
breaths using bag valve mask.
Check for proper placement during these first two
ventilations by:
-
Observing for bilateral rise and fall of the chest with each ventilation.
-
Observe the ET tube for misting, fogging, or condensation.
-
Auscultate for bilateral breath sounds:
Bilateral breath sounds present -
the ET tube has been properly placed causing both lungs to inflate with each
ventilation.
Breath sounds in right lung field only - the ET tube
has been placed too far down the bronchial tree and is in the right mainstem
bronchus. Pull back the endotracheal tube ¼ - ½ inch or until bilateral breath
sounds have been established.
h.
Secure Dressing (see figure 6)
-
Suture the ET tube in place (if required).
- Apply
petroleum gauze dressing to insertion site.
- Apply
dry sterile dressing over the insertion site.
-
Continue to ventilate patient (1 breath every 5 seconds) and suction as
necessary.

Substitute Figure
6.
Dressing for Emergency Cricothyroidotomy* |
i.
Monitor and reassess patient
-
Maintain ABC’s
-
Monitor and CASEVAC
6.
COMPLICATIONS ASSOCIATED WITH EMERGENCY
CRICOTHYROIDOTOMY
Hemorrhage - The most common complication
Causes
- Minor
bleeding may be caused by lacerating superficial capillaries in the skin.
- Significant bleeding may be caused by the laceration of major
vessels (carotid arteries and the jugular veins) within the neck.
Treatment
- Minor bleeding is treated with direct pressure and the
application of a simple pressure dressing.
- Significant bleeding - treated same as minor. However, if
unable to control the bleeding, the vessel may need to be ligated (tied off).
Esophageal Perforation or Tracheoesophageal Fistula
Definition - the creation of a hole between the
esophagus and trachea.
Causes
-
Creating an incision too deep through the cricothyroid membrane.
- Forcing the ET tube through the cricothyroid membrane and into
the esophagus.
Treatment - requires surgical repair at higher echelon
of care.
Subcutaneous emphysema
Definition - the presence of free air or gas within
the subcutaneous tissues. Upon palpation, a crackling sensation may be felt as
the air is pushed through the tissue.
Causes
- Creating too wide of an incision will allow air entrapment
under the skin.
- Air leaking out of the insertion site may get trapped under the
skin.
Treatment
-
No treatment is necessary. The subcutaneous emphysema will resolve
spontaneously within a few days.
- The
placement of petroleum gauze dressing around the incision/insertion site will
help reduce the incidence of subcutaneous emphysema.
|
CASUALTY
ASSESSMENT AND EMERGENCY CRICOTHYROIDOTOMY |
|
Care Under Fire
Phase: In the absence of life-threatening hemorrhage, there is no care
given for a casualty who needs a surgical cricothyroidotomy in this phase.
Tactical Field Care
Phase: Cricothyroidotomy is a skill you may use during Tactical Field
Care Phase. The need to perform an emergency cricothyroidotomy is made
after you have attempted to control the airway with other, less invasive
methods (i.e., NPA). Remember, once the patient has received a
cricothyroidotomy, they are now totally dependent upon you and now become
much more difficult to manage in a tactical environment. Complete a head
to toe assessment using DCAP-BTLS noting and treating additional
injuries. Determine if vascular access is required (see Combat Fluid
Resuscitation lesson) and give fluids if necessary. It is unlikely the
casualty will be able to drink fluids. Consider pain medications and give
antibiotics if warranted. Reassess all care provided. Document care
given, prevent hypothermia, and CASEVAC. |
REFERENCES
Pre-Hospital Trauma Life
Support, Military Edition, 6th Ed, Chapter 10
Emergency Procedures and Techniques, 3rd Ed
REV: July 2008
|
FMST: |
PERFORMANCE TEST |
|
TASK: |
EMERGENCY CRICOTHYROIDOTOMY |
|
DIRECTIONS: |
Without the aid of
references and given a simulated casualty and standard field medical
equipment and supplies, perform an emergency cricothyroidotomy
(FMST-HSS-1418g). |
|
This test
evaluates your ability to demonstrate the skills you were taught in
Emergency Cricothyroidotomy. You will be required to perform the
task on a mannequin and answer oral questions with regard to the
procedure.
Safety
considerations for this test include your ability to demonstrate or
verbalize universal precautions and maintain proper “sharps”
handling procedures, as you would be required to do in any patient
care situation.
There is
no time limit. Should you fail this evolution, you will be
remediated and retested until you master the skill. You will be
given three opportunities to complete this test. |
|
No. |
Your performance
will be evaluated using the following items: |
YES |
NO |
|
1. |
MAKE YOUR
DECISION |
|
|
|
|
Look, listen,
feel, attempt to ventilate
Justify your
decision |
□
□ |
□
□ |
|
2. |
ASSEMBLE AND
CHECK GEAR |
|
|
|
|
ET tube
Blade package
integrity
Betadine and
bandage packaging integrity
AMBU bag
(operation and fittings) |
□
□
□
□ |
□
□
□
□ |
|
3. |
PREPARE PATIENT |
|
|
|
|
Place patient
on back using C-spine control PRN
Explain
procedure to conscious patient |
□
□ |
□
□ |
|
4. |
LOCATE
ANATOMICAL LANDMARKS |
|
|
|
|
Palpate
thyroid and cricoid cartilage for orientation
Locate
cricothyroid membrane
Cleanse area |
□
□
□ |
□
□
□ |
|
5. |
MAKE INCISION |
|
|
|
|
Stabilize
thyroid cartilage
Use #11 blade
and make incision
Enter
cricothyroid membrane (either blunt dissect or incise) |
□
□
□ |
□
□
□ |
|
6. |
OPEN INCISION |
|
|
|
|
Either using
Kelly hemostat or knife blade handle |
□ |
□ |
|
7. |
INSERT TUBE |
|
|
|
|
Maintaining
control of trachea, pass the ET into trachea
Inflate
balloon and check for placement
Student must
verbalize indications of spontaneous breathing |
□
□
□ |
□
□
□ |
|
8. |
OCCLUSIVE
DRESSING |
|
|
|
|
Dress opening
and secure |
□ |
□ |
|
9. |
CASEVAC |
|
|
|
|
Student states
patient will be CASEVAC’ed |
□ |
□ |
|
STUDENT’S NAME AND PLATOON |
DATE |
ATTEMPT # |
INSTRUCTOR SIGNATURE
|
|
INSTRUCTOR’S
COMMENTS: |
| |
|
|
|
|
|
|
|
Cricothyroidotomy Review
1. List two advantages of
performing a cricothyroidotomy.
2. List the nine steps in
performing an emergency cricothyroidotomy.
3. Identify
the most common complication from performing an emergency cricothyroidotomy.
4. Why is petroleum gauze used in
securing the site? |
*The FMST Student
Manual was produced by the Field Medical Training Battalion-East, Camp Lejeune,
North Carolina. This 2008 web edition has been enhanced by the Brookside
Associates, Ltd., preserving all of the original text material, while
augmenting, modifying, eliminating or replacing some of the graphics to comply with
privacy and copyright laws, and to enhance the training value. These
enhancements are marked with a red box
□
and are C. 2008, with all rights
reserved.
|
|