High Altitude Burst
Characteristics
Detonation of a weapon at an
altitude above 100,000 ft
Fireball is much larger and
expands much more rapidly than a surface or subsurface burst
Ionizing radiation can
travel for hundreds of miles before being absorbed
Causes severe disruption in communication and leads to an
electromagnetic pulse (EMP), which can significantly degrade or destroy
electronic and critical medical equipment
Air Burst
Characteristics
An explosion in which a
weapon is detonated at an altitude below 100,000 feet but high enough that the
fireball does not contact the surface of the earth
Airbursts may cause
considerable damage; thermal burns to exposed skin may be produced many
kilometers away from the burst.
Eye injuries may be produced
at even a much greater distance than that of thermal burns.
Tactically, airbursts are the most likely to be used against
ground forces.
Surface Burst
Characteristics
An explosion in which a
weapon is detonated on or slightly above the surface of the earth so that the
fireball actually touches the land or water surface.
The area affected by the
blast, thermal radiation, and initial nuclear radiation will be less extensive
than an air burst of similar yield
It produces the greatest
amount of fallout over a much larger area than that which is affected by blast
and thermal radiation
Subsurface Burst
Characteristics
An explosion in which the
point of detonation is beneath the surface of land or water
Cratering of the ground will
generally result
If the subsurface burst does
not penetrate the surface, the only other hazard will be from ground or water
shock
If the burst is shallow
enough to penetrate the surface, blast, thermal and initial nuclear radiation
effects will be present, but less than a surface burst of comparable yield
If the burst penetrates the
surface, fallout will be heavy
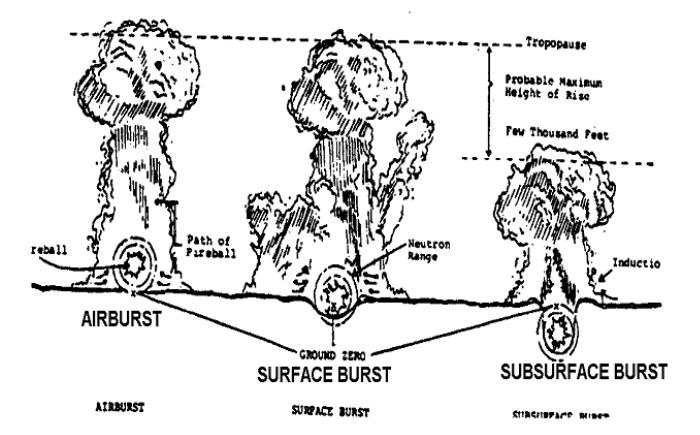
Figure
1. Types of Nuclear Blasts
4. COMMON
TYPES OF NUCLEAR INJURIES
Two Types of Blast Injuries:
Although there are many
effects of a standard blast (see block 4 “Blast Injuries”) the following
information divides the types of injuries that may result from a nuclear
explosion into two types, primary and secondary.
Primary Blast Injury
(Direct)
- these
types of injuries are caused by the direct action of the shock wave on the human
body after the detonation of a nuclear device.
Injuries occur immediately
after detonation due to over pressure from rapid the expansion of air.
If the patient is in close
proximity to ground zero, the initial blast wave is usually lethal.
Sub lethal exposures to the initial blast wave can result in
damage to bones, muscles, lungs, gastrointestinal system and ruptured eardrums.
Secondary Blast Injury (Indirect)
- these injuries are caused by indirect wind forces greater than several
kilometers per hour seconds after the primary detonation of a nuclear device.
Injuries occur as a result
of collapsing buildings, flying timber and other debris impacting the body or
physical displacement of the body against objects or structures.
More injuries are caused by
indirect blast wind drag forces than by the shock wave.
Treatment of Blast Injuries from a Nuclear Attack:
Blunt
trauma - blunt trauma with nuclear detonation will be
anywhere from mild to severe. Injuries occur as a result of debris put into
motion from blast and its following winds. Injuries such as fractures, spinal
injury, head and torso blunt trauma, and penetrating injuries should be
expected. Care for these injuries as you would in a non-contaminated
environment.
